Sleep Apnea Clues You Might Miss: When to Book an ENT Clinic Assessment

Not Just Snoring: Subtle Sleep Apnea Signs an ENT Doctor Looks For
Many people associate sleep apnea with loud snoring and obvious breathing pauses. But in real life, it often shows up in quieter, easily dismissed ways—morning headaches, a foggy brain, “mystery” fatigue, or waking up more tired than when you went to bed. Some people don’t even think they snore. Others do snore, but assume it’s harmless, especially if they’re otherwise healthy and busy.
Sleep apnea matters because it is not just a sleep issue—it can affect your heart health, blood pressure, mood, metabolism, and safety (especially if you drive or operate machinery while exhausted). The good news is that the right assessment can reveal what’s happening and open the door to treatment that genuinely improves daily life.
An ENT clinic assessment is often the missing step when symptoms are confusing, snoring is dismissed, or nasal and throat factors may be contributing to airway obstruction.
What Sleep Apnea Actually Is (and Why It’s Missed)
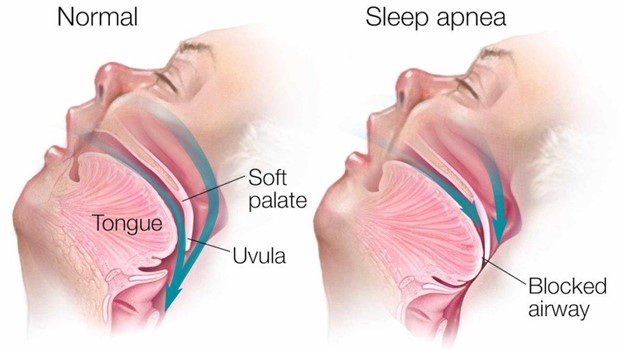
Sleep apnea—most commonly obstructive sleep apnea (OSA)—occurs when the upper airway narrows or collapses during sleep. Breathing becomes shallow (hypopnea) or stops briefly (apnea). Your oxygen levels can drop, and your brain partially wakes you up to reopen the airway. Many people don’t remember these micro-awakenings, but they fragment sleep all night.
That’s why someone can sleep for 7–8 hours and still feel drained: they’re not getting stable, restorative sleep.
Sleep apnea is missed because:
- Symptoms can be non-specific (fatigue, headaches, irritability)
- Snoring may not be loud or may be unnoticed.
- People assume stress, ageing, or “busy life” is the cause
- Partners notice issues first (or there may be no partner to observe sleep)
Sleep Apnea Clues You Might Miss
1) You’re tired, but not in an “I didn’t sleep enough” way
Sleep apnea fatigue often feels like:
- heavy eyelids by mid-morning
- brain fog and slower thinking
- needing caffeine to feel normal
- energy crashes, especially after lunch
- feeling unrefreshed even after a long night
This is different from a late-night tiredness. It’s the kind that follows you.
2) Morning headaches or a “pressure” feeling in the head
Waking headaches can come from sleep fragmentation and oxygen changes overnight. If you repeatedly wake with headaches—especially alongside snoring or poor sleep—sleep apnea becomes more likely.

3) Dry mouth, sore throat, or thirst on waking
Many people with OSA breathe through the mouth during sleep because the nose is blocked or the airway is constricted. Common signs include:
- waking with a dry mouth
- sore throat without infection
- needing water immediately upon waking
4) Night-time urination (more than you’d expect)
Waking to pass urine can be caused by multiple factors, but frequent night-time trips—especially with snoring and daytime tiredness—can be a clue. Sleep apnea can affect hormones involved in fluid balance overnight.
5) Mood changes that look like stress (or “just life”)
Sleep apnea can quietly affect:
- irritability
- low mood
- anxiety-like restlessness
- reduced motivation
- shorter emotional fuse
If you’re doing “all the right things” but still feel off, sleep quality is worth investigating.
6) Poor concentration and memory slips
If you’re:
- reading the same line twice
- forgetting small tasks
- struggling with focus in meetings
- making more mistakes than usual
…sleep fragmentation may be the hidden factor.
7) Reflux-like symptoms at night
Some people with sleep apnea notice:
- throat irritation
- chronic cough
- hoarseness in the morning
- reflux sensations at night
It’s not that reflux always means apnea, but sleep-related airway strain can overlap with throat symptoms.
8) Restless sleep, sweating, or waking with a racing heart
You might not notice breathing pauses, but you may notice:
- tossing and turning
- waking suddenly, feeling alert
- sweating despite a cool room
- palpitations on waking
These can reflect repeated stress responses during the night.
9) “Silent snoring” signs your partner notices
A partner may report:
- breathing pauses
- gasping or choking sounds
- snoring that stops and starts
- restless movement
- Are you sleeping better on your side than on your back?
Even if you’re not aware, partner observations are valuable clinical clues.
10) Teeth grinding or jaw tension
Some people clench or grind during fragmented sleep. If your dentist has mentioned bruxism, and you’re also tired of snoring or morning headaches, it’s worth considering OSA as part of the picture.
11) High blood pressure that’s new, difficult to control, or “unexplained”.
Sleep apnea is linked with elevated blood pressure and cardiovascular strain. If you’ve developed hypertension or your readings remain high despite lifestyle efforts, checking for sleep apnea is sensible.
12) You doze off easily in “quiet moments”.
If you:
- nod off while watching TV
- struggle to stay awake as a passenger in a car
feel sleepy in meetings
…that level of daytime sleepiness is a safety issue, not just an inconvenience.
When to Book an ENT Clinic Assessment
You don’t need to wait until symptoms are extreme. Book an ENT assessment if you have:
- loud, frequent snoring (especially with daytime fatigue)
- suspected breathing pauses, gasping, or choking during sleep
- morning headaches, dry mouth, and persistent tiredness
- chronic nasal blockage, sinus symptoms, or mouth breathing at night
- enlarged tonsils, frequent tonsillitis, or a “tight throat” feeling
- a history of deviated septum, nasal polyps, or persistent rhinitis
- failed “quick fixes” (nasal strips, sprays, mouth taping, sleep gadgets)
- high blood pressure, type 2 diabetes risk, or weight gain with worsening fatigue
- significant daytime sleepiness affecting driving or work
An ENT assessment is especially helpful when anatomy and airflow may be contributing—nose, palate, tonsils, tongue base, or jaw structure.
What Happens in an ENT Sleep Apnea Assessment
A symptom and risk review
A sleep apnea doctor will ask about:
- snoring frequency and pattern
- witnessed apneas (partner reports)
- daytime sleepiness and concentration
- alcohol and sedative use (these can worsen airway collapse)
- nasal obstruction, allergies, sinus history
- reflux symptoms and throat irritation
- medical risk factors such as hypertension
You may also be asked to complete a short sleepiness questionnaire to quantify symptoms.
Physical examination (nose, throat, airway)
ENT assessment focuses on structures that influence airflow:
- nasal septum alignment and turbinate swelling
- signs of allergies or chronic rhinitis
- tonsil size and throat space
- soft palate position
- tongue size and jaw relationship
- neck circumference and airway shape
Nasal endoscopy (when needed)
A nose scope procedure (Nasoendoscopy) may be used to assess:
- nasal blockage from polyps or swelling
- adenoid tissue (in some cases)
- throat anatomy related to obstruction

Recommendation for a sleep study
A sleep study is what confirms sleep apnea and measures severity. Depending on your symptoms and risk profile, your clinician may recommend:
- home sleep apnea testing (in selected cases)
- in-lab polysomnography (more detailed)
The key is objective confirmation—because treatment choice depends on severity and pattern.
Red Flags: Don’t Delay Assessment
Seek prompt medical review if you have:
- Falling asleep while driving or at work
- Loud snoring with witnessed apneas
- Severe daytime sleepiness affecting safety
- Morning chest tightness, breathlessness, or significant palpitations
- Uncontrolled high blood pressure with sleep symptoms
- New or worsening headaches with severe sleep disruption
Treatment Options (What the ENT Path Can Unlock)
ENT-led care doesn’t mean “straight to surgery.” It means you get a targeted plan based on the cause and severity.
Lifestyle and sleep-position strategies
For mild cases, improvements can come from:
- weight management (when relevant)
- side sleeping (for position-dependent OSA)
- Reducing alcohol close to bedtime
- optimising sleep routines
CPAP therapy
CPAP is a common and highly effective treatment for many people. It keeps the airway open with gentle air pressure. When tolerated well, it can dramatically reduce symptoms and health risks.
Oral appliances (in suitable candidates)
Dental sleep appliances can reposition the jaw to keep the airway open, often used in mild to moderate OSA or when CPAP isn’t tolerated.
Addressing nasal blockage
If nasal obstruction is a major factor, treating it can improve sleep quality and make CPAP easier to tolerate. Treatment may include:
- nasal steroid sprays and allergy management
- saline irrigation
- selected procedures for structural blockage (when appropriate)
Targeted ENT procedures (when indicated)
For selected patients, procedures may address specific anatomical obstruction—particularly if tonsils or other structures are contributing. The right option depends on your anatomy, severity, and sleep study results.
How to Prepare for Your ENT Appointment
Bring:
- a short symptom timeline (when it started, what worsened it)
- any partner observations (pauses, gasps, restlessness)
- a list of medications and supplements
- prior reports (sinus scans, nasal surgery history, allergy testing, if any)
- blood pressure readings if relevant
If possible, record a short snoring clip (audio) to show the pattern—many clinicians find it helpful.
The Takeaway: Subtle Clues Deserve Serious Attention
Sleep apnea isn’t always obvious. You don’t need dramatic choking episodes to justify an assessment—often the earliest clues are quiet: persistent fatigue, morning headaches, dry mouth, brain fog, mood changes, and “unexplained” sleep disruption.
If these symptoms are affecting your day-to-day life, an ENT clinic assessment can clarify whether nasal or throat factors are contributing and guide you towards the right next step—often a sleep study and a treatment plan that helps you wake up feeling like yourself again.